Control blood pressure to below 150/80 mm Hg
The UKPDS also compared tight blood pressure control (aiming at systolic <150 mm Hg and diastolic <80) with usual treatment. Tight control reduced relative deaths attributed to diabetes by 32% (NNT=150 patient-years), and demonstrated a trend toward reduced total mortality that was not statistically significant (relative risk reduction [RRR]=18%; 95% confidence interval [CI], –0.8% to 37%). Both stroke (NNT=196 patient-years) and the aggregate endpoint of “all microvascular disease” (NNT=139 patient-years) were significantly reduced by tight blood pressure control.10
The Hypertension Optimal Treatment (HOT) Study Group11 compared various levels of blood pressure control. A reduction in cardiovascular mortality was significant even between those treated with a goal of 80 and 85 mm Hg diastolic (RRR=67%; NNT=133 patient-years). The trend toward reduction in total mortality in this trial also approached statistical significance (P=.068; RRR=42%).
The Syst-Eur trial13 compared tight blood pressure control on nitrendipine with looser control with a variety of agents. Cardiovascular mortality was reduced by 30% with tight control (NNT=100 patient-years).
The Heart Outcomes Prevention Evaluation (HOPE) study6 included patients with diabetes, of which only 56% had a diagnosis of hypertension. It randomized participants to receive ramipril or placebo, in addition to any off-study antihypertensive agents they were already using. The intervention group had both lower average blood pressures as well as lower total mortality by 24% (NNT=140 patient-years).
Impact of type 2 diabetes
Type 2 diabetes is the second most common problem seen by family physicians, and represents over 4% of office visits.19 The cost to society is staggering: in the United States, $100 billion was spent in 1997 alone.20 Its toll in clinical outcomes is also dramatic, leading to over 150,000 annual deaths in the US.20
Left unchecked, diabetes leads to microvascular and macrovascular complications. Cardiovascular disease occurs 2 to 3 times more often among patients with diabetes than healthy individuals,21,22 and is also linked to impaired glucose tolerance.23 Cardiovascular events are responsible for over half of deaths in patients with diabetes.20
Each year, neuropathy contributes to ulcers in 2% of patients with diabetes, and amputation in 0.6%.24 Proteinuria occurs in 20% to 40% of all patients with diabetes7; of those, 20% rapidly develop end-stage renal disease.25 Retinopathy is treated at a rate of 1% per year among patients with diabetes.14
Choice of agent important. Lower blood pressure goals have consistently demonstrated benefit across multiple studies. The choice of antihypertensive agent may also affect outcomes (Table 3). The UKPDS blood pressure analysis was also stratified to evaluate whether the results of blood pressure treatment differed between captopril and atenolol. Though compliance was slightly better with captopril, there were no differences in patient-oriented outcomes between the groups.26
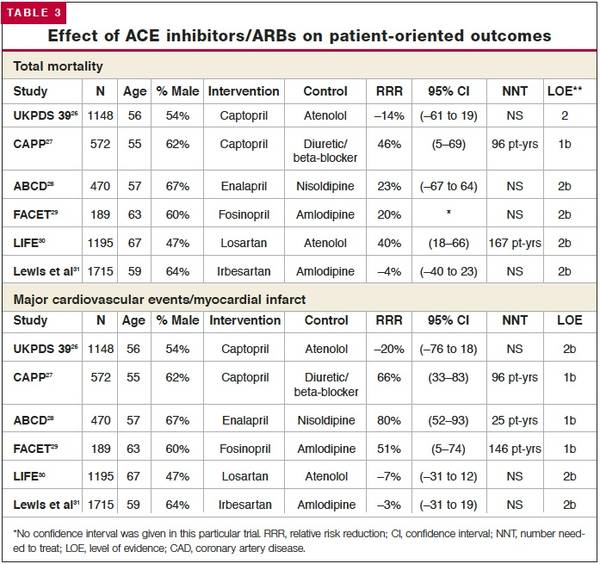
The Captopril Prevention Project (CAPPP)27 compared captopril with diuretics and betablockers alone or in combination. While blood pressure control was about the same in all study groups, the captopril group realized a 66% reduction in MI (NNT=96 patient-years) and a total mortality 46% less than that seen with the other agents (NNT=96 patient-years).
The Appropriate Blood Pressure Control in Diabetes (ABCD) trial28 compared nisoldipine and enalapril. Participants randomized to receive the ACE inhibitor had an 80% decreased risk of MI (NNT=25 patient-years).
In the Fosinopril versus Amlodipine Cardiovascular Events Trial (FACET),29 blood pressure was better controlled with amlodipine, but major vascular events were 51% fewer with the ACE inhibitor (NNT=146 patient-years), again supporting the superior performance of ACE inhibitors.
Angiotensin receptor blockers (ARBs) may have comparable effects to ACE inhibitors. The Losartan Intervention For Endpoint Reduction in Hypertension (LIFE) trial30 studied patients with left ventricular hypertrophy, diabetes, and hypertension, comparing losartan with atenolol. Total mortality with losartan was reduced by a relative 40% compared with atenolol (NNT=167 patientyears). Another study31 of patients with diabetes, hypertension, and nephropathy compared irbesartan with amlodipine. This trial demonstrated no differences in patient-oriented outcomes between the calcium-channel blocker and the ARB.
Applying the evidence. The goals for blood pressure control in type 2 diabetes should be less than 150 mm Hg systolic and 80 mm Hg diastolic (SOR: A). Evidence also strongly supports the use of an ACE inhibitor, or possibly ARB, as first-linetreatment for hypertension in diabetes (SOR: A). Many authorities recommend even more aggressive blood pressure goals.
Lipid management: statins improve outcome
Lowering elevated triglycerides has not been independently associated with an improvement in patient-oriented outcomes. In the Helsinki Heart Study22 and the St. Mary’s, Ealing, Northwick Park Diabetes Cardiovascular Disease Prevention (SENDCAP) trial,32 a fibric acid derivative was compared with placebo. The average triglyceride concentration was decreased, but no significant effect on coronary events was noted. However, elevated triglycerides are associated with the metabolic syndrome, which may warrant lifestyle changes or medication (based on expert opinion).